
In Axing mRNA Contract, Trump Delivers Another Blow to US Biosecurity, Former Officials Say
The Trump administration’s cancellation of $766 million in contracts to develop mRNA vaccines against potential pandemic flu viruses is the latest blow to national defense, former health security officials said. They warned that the U.S. could be at the mercy of other countries in the […]
Pharmaceuticals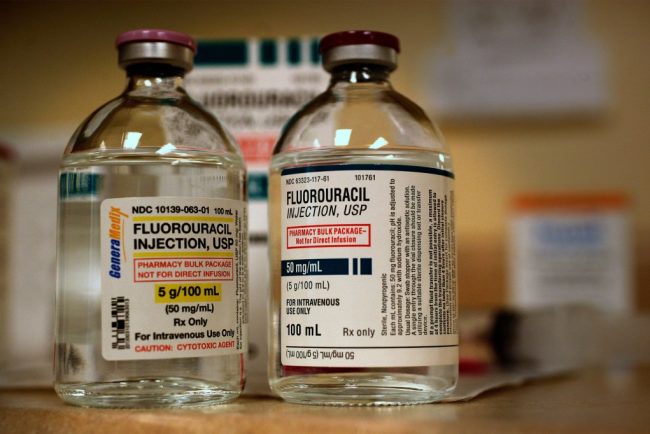
Two Patients Faced Chemo. The One Who Survived Demanded a Test To See if It Was Safe.
JoEllen Zembruski-Ruple, while in the care of New York City’s renowned Memorial Sloan Kettering Cancer Center, swallowed the first three chemotherapy pills to treat her squamous cell carcinoma on Jan. 29, her family members said. They didn’t realize the drug could kill her. Six days […]
Pharmaceuticals
Trump Exaggerates Speed and Certainty of Prescription Drug Price Reductions
Under a new executive order, prescription drug prices will be reduced “almost immediately.” President Donald Trump, in a May 11 post on Truth Social President Donald Trump expressed high hopes for an executive order to reduce drug prices. On May 11, the day before he […]
Pharmaceuticals





In Axing mRNA Contract, Trump Delivers Another Blow to US Biosecurity, Former Officials Say
The Trump administration’s cancellation of $766 million in contracts to develop mRNA vaccines against potential pandemic flu viruses is the latest blow to national defense, former health security officials said. They warned that the U.S. could be at the mercy of other countries in the […]
Pharmaceuticals Two Patients Faced Chemo. The One Who Survived Demanded a Test To See if It Was Safe.
JoEllen Zembruski-Ruple, while in the care of New York City’s renowned Memorial Sloan Kettering Cancer Center, swallowed the first three chemotherapy pills to treat her squamous cell carcinoma on Jan. 29, her family members said. They didn’t realize the drug could kill her. Six days […]
PharmaceuticalsJoEllen Zembruski-Ruple, while in the care of New York City’s renowned Memorial Sloan Kettering Cancer Center, swallowed the first three chemotherapy pills to treat her squamous cell carcinoma on Jan. 29, her family members said. They didn’t realize the drug could kill her.
Six days later, Zembruski-Ruple went to Sloan Kettering’s urgent care department to treat sores in her mouth and swelling around her eyes. The hospital diagnosed oral yeast infection and sent her home, her sister and partner said. Two days later, they said, she returned in agony — with severe diarrhea and vomiting — and was admitted. “Enzyme deficiency,” Zembruski-Ruple texted a friend.
The 65-year-old, a patient advocate who had worked for the National Multiple Sclerosis Society and other groups, would never go home.
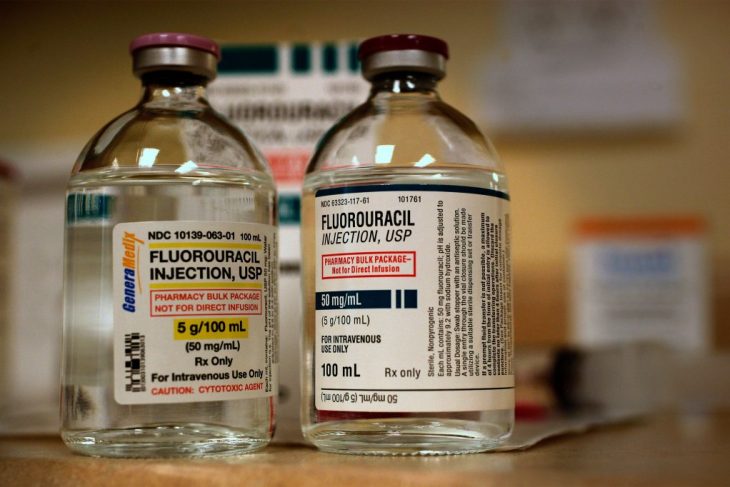
Covered in bruises and unable to swallow or talk, she eventually entered hospice care and died March 25 from the very drug that was supposed to extend her life, said her longtime partner, Richard Khavkine. Zembruski-Ruple was deficient in the enzyme that metabolizes capecitabine, the chemotherapy drug she took, said Khavkine and Susan Zembruski, one of her sisters. Zembruski-Ruple was among about 1,300 Americans each year who die from the toxic effects of that pill or its cousin, the IV drug fluorouracil known as 5-FU.

Doctors can test for the deficiency — and then either switch drugs or lower the dosage if patients have a genetic variant that carries risk. The FDA approved an antidote in 2015, but it’s expensive and must be administered within four days of the first chemotherapy treatment.
Newer cancer drugs sometimes include a companion diagnostic to determine whether a drug works with an individual patient’s genetics. But 5-FU went on the market in 1962 and sells for about $17 a dose; producers of its generic aren’t seeking approval for toxicity tests, which typically cost hundreds of dollars. Doctors have only gradually understood which gene variants are dangerous in which patients, and how to deal with them, said Alan Venook, a colorectal and liver cancer specialist at the University of California-San Francisco.
By the time Zembruski-Ruple’s doctors told her she had the deficiency, she had been on the drug for eight days, said Khavkine, who watched over his partner with her sister throughout the seven-week ordeal.
Khavkine said he “would have asked for the test” if he had known about it, but added “nobody told us about the possibility of this deficiency.” Zembruski-Ruple’s sister also said she wasn’t warned about the fatal risks of the chemo, or told about the test.
“They never said why they didn’t test her,” Zembruski said. “If the test existed, they should have said there is a test. If they said, ‘Insurance won’t cover it,’ I would have said, ‘Here’s my credit card.’ We should have known about it.”
Guidance Moves at a Glacial Pace
Despite growing awareness of the deficiency, and an advocacy group made up of grieving friends and relatives who push for routine testing of all patients before they take the drug, the medical establishment has moved slowly.
A panel of the National Comprehensive Cancer Network, or NCCN — specialists from Sloan Kettering and other top research centers — until recently did not recommend testing, and the FDA does not require it.
In response to a query from KFF Health News about its policy, Sloan Kettering spokesperson Courtney Nowak said the hospital treats patients “in accordance with NCCN guidelines.” She said the hospital would not discuss a patient’s care.
On Jan. 24, the FDA issued a warning about the enzyme deficiency in which it urged health care providers to “inform patients prior to treatment” about the risks of taking 5-FU and capecitabine.
On March 31 — six days after Zembruski-Ruple’s death — the network’s expert panel for most gastrointestinal cancers took a first step toward recommending testing for the deficiency.
Worried that President Donald Trump’s FDA might do nothing, Venook said, the panel — whose guidance shapes the practices of oncologists and health insurers — recommended that doctors consider testing before dosing patients with 5-FU or capecitabine.
However, its guidance stated that “no specific test is recommended at this time,” citing a lack of data to “inform dose adjustments.”
Sloan Kettering “will consider this guidance in developing personalized treatment plans for each patient,” Nowak told KFF Health News.
The new NCCN guidance was “not the blanket recommendation we were working toward, but it is a major step toward our ultimate goal,” said Kerin Milesky, a public health official in Brewster, Massachusetts, who’s part of an advocacy group for testing. Her husband, Larry, died two years ago at age 73 after a single treatment of capecitabine.
European drug regulators began urging oncologists to test patients for deficiency in May 2020. Patients with potentially risky genetics are started on a half-dose of the cancer drug. If they suffer no major toxicity, the dose is increased.
A Lifesaving Ultimatum?
Emily Alimonti, a 42-year-old biotech salesperson in upstate New York, chose that path before starting capecitabine treatment in December. She said her doctors — including an oncologist at Sloan Kettering — told her they didn’t do deficiency testing, but Alimonti insisted. “Nope,” she said. “I’m not starting it until I get the test back.”
The test showed that Alimonti had a copy of a risky gene variant, so doctors gave her a lower dose of the drug. Even that has been hard to tolerate; she’s had to skip doses because of low white blood cell counts, Alimonti said. She still doesn’t know whether her insurer will cover the test.

Around 300,000 people are treated with 5-FU or capecitabine in the United States each year, but its toxicity could well have prevented FDA approval were it up for approval today. Short of withdrawing a drug, however, U.S. regulators have little power to manage its use. And 5-FU and capecitabine are still powerful tools against many cancers.
At a January workshop that included FDA officials and cancer specialists, Venook, the NCCN panel’s co-chair, asked whether it was reasonable to recommend that doctors obtain a genetic test “without saying what to do with the result.”
But Richard Pazdur, the FDA’s top cancer expert, said it was time to end the debate and commence testing, even if the results could be ambiguous. “If you don’t have the information, how do you have counseling?” he asked.
Two months later, Venook’s panel changed course. The price of tests has fallen below $300 and results can be returned as soon as three days, Venook said. Doubts about the FDA’s ability to further confront the issue spurred the panel’s change of heart, he said.
“I don’t know if FDA is going to exist tomorrow,” Venook told KFF Health News. “They’re taking a wrecking ball to common sense, and that’s one of the reasons we felt we had to go forward.”
On May 20, the FDA posted a Federal Register notice seeking public input on the issue, a move that suggested it was considering further action.
Venook said he often tests his own patients, but the results can be fuzzy. If the test finds two copies of certain dangerous gene variants in a patient, he avoids using the drug. But such cases are rare — and Zembruski-Ruple was one of them, according to her sister and Khavkine.
Many more patients have a single copy of a suspect gene, an ambiguous result that requires clinical judgment to assess, Venook said.
A full-gene scan would provide more information but adds expense and time, and even then the answer may be murky, Venook said. He worries that starting patients on lower doses could mean fewer cures, especially for newly diagnosed colon cancer patients.
Power Should Rest With Patients
Scott Kapoor, a Toronto-area emergency room physician whose brother Anil, a much-loved urologist and surgeon, died of 5-FU toxicity at age 58 in 2023, views Venook’s arguments as medical paternalism. Patients should decide whether to test and what to do with the results, he said.
“What’s better — don’t tell the patient about the test, don’t test them, potentially kill them in 20 days?” he said. “Or tell them about the testing while warning that potentially the cancer will kill them in a year?”
“People say oncologists don’t know what to do with the information,” said Karen Merritt, whose mother died after an infusion of 5-FU in 2014. “Well, I’m not a doctor, but I can understand the Mayo Clinic report on it.”
The Mayo Clinic recommends starting patients on half a dose if they have one suspect gene variant. And “the vast majority of patients will be able to start treatment without delays,” Daniel Hertz, a clinical pharmacologist from the University of Michigan, said at the January meeting.
Some hospitals began testing after patients died because of the deficiency, said Lindsay Murray, of Andover, Massachusetts, who has advocated for widespread testing since her mother was treated with capecitabine and died in 2021.
In some cases, Venook said, relatives of dead patients have sued hospitals, leading to settlements.
Kapoor said his brother — like many patients of non-European origin — had a gene variant that hasn’t been widely studied and isn’t included in most tests. But a full-gene scan would have detected it, Kapoor said, and such scans can also be done for a few hundred dollars.
The cancer network panel’s changed language is disappointing, he said, though “better than nothing.”
In video tributes to Zembruski-Ruple, her friends, colleagues, and clients remembered her as kind, helpful, and engaging. “JoEllen was beautiful both inside and out,” said Barbara McKeon, a former colleague at the MS Society. “She was funny, creative, had a great sense of style.”
“JoEllen had this balance of classy and playful misbehavior,” psychotherapist Anastatia Fabris said. “My beautiful, vibrant, funny, and loving friend JoEllen.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
Trump Exaggerates Speed and Certainty of Prescription Drug Price Reductions
Under a new executive order, prescription drug prices will be reduced “almost immediately.” President Donald Trump, in a May 11 post on Truth Social President Donald Trump expressed high hopes for an executive order to reduce drug prices. On May 11, the day before he […]
Pharmaceuticals
How Trump Aims To Slash Federal Support for Research, Public Health, and Medicaid
Health care has proved a vulnerable target for the firehose of cuts and policy changes President Donald Trump ordered in the name of reducing waste and improving efficiency. But most of the impact isn’t as tangible as, say, higher egg prices at the grocery store. […]
Pharmaceuticals
Pharmacists Stockpile Most Common Drugs on Chance of Targeted Trump Tariffs
In the dim basement of a Salt Lake City pharmacy, hundreds of amber-colored plastic pill bottles sit stacked in rows, one man’s defensive wall in a tariff war. Independent pharmacist Benjamin Jolley and his colleagues worry that the tariffs, aimed at bringing drug production to […]
PharmaceuticalsIn the dim basement of a Salt Lake City pharmacy, hundreds of amber-colored plastic pill bottles sit stacked in rows, one man’s defensive wall in a tariff war.
Independent pharmacist Benjamin Jolley and his colleagues worry that the tariffs, aimed at bringing drug production to the United States, could instead drive companies out of business while raising prices and creating more of the drug shortages that have plagued American patients for several years.
Jolley bought six months’ worth of the most expensive large bottles, hoping to shield his business from the 10% across-the-board tariffs on imported goods that President Donald Trump announced April 2. Now with threats of additional tariffs targeting pharmaceuticals, Jolley worries that costs will soar for the medications that will fill those bottles.
In principle, Jolley said, using tariffs to push manufacturing from China and India to the U.S. makes sense. In the event of war, China could quickly stop all exports to the United States.
“I understand the rationale for tariffs. I’m not sure that we’re gonna do it the right way,” Jolley said. “And I am definitely sure that it’s going to raise the price that I pay my suppliers.”
Squeezed by insurers and middlemen, independent pharmacists such as Jolley find themselves on the front lines of a tariff storm. Nearly everyone down the line — drugmakers, pharmacies, wholesalers, and middlemen — opposes most tariffs.
Slashing drug imports could trigger widespread shortages, experts said, because of America’s dependence on Chinese- and Indian-made chemical ingredients, which form the critical building blocks of many medicines. Industry officials caution that steep tariffs on raw materials and finished pharmaceuticals could make drugs more expensive.
“Big ships don’t change course overnight,” said Robin Feldman, a UC Law San Francisco professor who writes about prescription drug issues. “Even if companies pledge to bring manufacturing home, it will take time to get them up and running. The key will be to avoid damage to industry and pain to consumers in the process.”
Trump on April 8 said he would soon announce “a major tariff on pharmaceuticals,” which have been largely tariff-free in the U.S. for 30 years.
“When they hear that, they will leave China,” he said. The U.S. imported $213 billion worth of medicines in 2024 — from China but also India, Europe, and other areas.
Trump’s statement sent drugmakers scrambling to figure out whether he was serious, and whether some tariffs would be levied more narrowly, since many parts of the U.S. drug supply chain are fragile, drug shortages are common, and upheaval at the FDA leaves questions about whether its staffing is adequate to inspect factories, where quality problems can lead to supply chain crises.
On May 12, Trump signed an executive order asking drugmakers to bring down the prices Americans pay for prescriptions, to put them in line with prices in other countries.
Meanwhile, pharmacists predict even the 10% tariffs Trump has demanded will hurt: Jolley said a potential increase of up to 30 cents a vial is not a king’s ransom, but it adds up when you’re a small pharmacy that fills 50,000 prescriptions a year.
“The one word that I would say right now to describe tariffs is ‘uncertainty,’” said Scott Pace, a pharmacist and owner of Kavanaugh Pharmacy in Little Rock, Arkansas.
To weather price fluctuations, Pace stocked up on the drugs his pharmacy dispenses most.

“I’ve identified the top 200 generics in my store, and I have basically put 90 days’ worth of those on the shelf just as a starting point,” he said. “Those are the diabetes drugs, the blood pressure medicines, the antibiotics — those things that I know folks will be sicker without.”
Pace said tariffs could be the death knell for the many independent pharmacies that exist on “razor-thin margins” — unless reimbursements rise to keep up with higher costs.
Unlike other retailers, pharmacies can’t pass along such costs to patients. Their payments are set by health insurers and pharmacy benefit managers largely owned by insurance conglomerates, who act as middlemen between drug manufacturers and purchasers.
Neal Smoller, who employs 15 people at his Village Apothecary in Woodstock, New York, is not optimistic.
“It’s not like they’re gonna go back and say, well, here’s your 10% bump because of the 10% tariff,” he said. “Costs are gonna go up and then the sluggish responses from the PBMs — they’re going to lead us to lose more money at a faster rate than we already are.”
Smoller, who said he has built a niche selling vitamins and supplements, fears that FDA firings will mean fewer federal inspections and safety checks.
“I worry that our pharmaceutical industry becomes like our supplement industry, where it’s the wild West,” he said.

Narrowly focused tariffs might work in some cases, said Marta Wosińska, a senior fellow at the Brookings Institution’s Center on Health Policy. For example, while drug manufacturing plants can cost $1 billion and take three to five years to set up, it would be relatively cheap to build a syringe factory — a business American manufacturers abandoned during the covid-19 pandemic because China was dumping its products here, Wosińska said.
It’s not surprising that giants such as Novartis and Eli Lilly have promised Trump they’ll invest billions in U.S. plants, she said, since much of their final drug product is made here or in Europe, where governments negotiate drug prices. The industry is using Trump’s tariff saber-rattling as leverage; in an April 11 letter, 32 drug companies demanded European governments pay them more or face an exodus to the United States.
Brandon Daniels, CEO of supply chain company Exiger, is bullish on tariffs. He thinks they could help bring some chemical manufacturing back to the U.S., which, when coupled with increased use of automation, would reduce the labor advantages of China and India.
“You’ve got real estate in North Texas that’s cheaper than real estate in Shenzhen,” he said at an economic conference April 25 in Washington, referring to a major Chinese chemical manufacturing center.
But Wosińska said no amount of tariffs will compel makers of generic drugs, responsible for 90% of U.S. prescriptions, to build new factories in the U.S. Payment structures and competition would make it economic suicide, she said.
Several U.S. generics firms have declared bankruptcy or closed U.S. factories over the past decade, said John Murphy, CEO of the Association for Accessible Medicines, the generics trade group. Reversing that trend won’t be easy and tariffs won’t do it, he said.
“There’s not a magic level of tariffs that magically incentivizes them to come into the U.S.,” he said. “There is no room to make a billion-dollar investment in a domestic facility if you’re going to lose money on every dose you sell in the U.S. market.”
His group has tried to explain these complexities to Trump officials, and hopes word is getting through. “We’re not PhRMA,” Murphy said, referring to the powerful trade group primarily representing makers of brand-name drugs. “I don’t have the resources to go to Mar-a-Lago to talk to the president myself.”
Many of the active ingredients in American drugs are imported. Fresenius Kabi, a German company with facilities in eight U.S. states to produce or distribute sterile injectables — vital hospital drugs for cancer and other conditions — complained in a letter to U.S. Trade Representative Jamieson Greer that tariffs on these raw materials could paradoxically lead some companies to move finished product manufacturing overseas.
Fresenius Kabi also makes biosimilars, the generic forms of expensive biologic drugs such as Humira and Stelara. The United States is typically the last developed country where biosimilars appear on the market because of patent laws.
Tariffs on biosimilars coming from overseas — where Fresenius makes such drugs — would further incentivize U.S. use of more expensive brand-name biologics, the March 11 letter said. Biosimilars, which can cost a tenth of the original drug’s price, launch on average 3-4 years later in the U.S. than in Canada or Europe.
In addition to getting cheaper knockoff drugs faster, European countries also pay far less than the United States for brand-name products. Paradoxically, Murphy said, those same countries pay more for generics.
European governments tend to establish more stable contracts with makers of generics, while in the United States, “rabid competition” drives down prices to the point at which a manufacturer “maybe scrimps on product quality,” said John Barkett, a White House Domestic Policy Council member in the Biden administration.
As a result, Wosińska said, “without exemptions or other measures put in place, I really worry about tariffs causing drug shortages.”
Smoller, the New York pharmacist, doesn’t see any upside to tariffs.
“How do I solve the problem of caring for my community,” he said, “but not being subject to the emotional roller coaster that is dispensing hundreds of prescriptions a day and watching every single one of them be a loss or 12 cents profit?”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).

KFF Health News' 'What the Health?': GOP Tries To Cut Billions in Health Benefits
The Host Julie Rovner KFF Health News @jrovner @julierovner.bsky.social Read Julie’s stories. Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the […]
PharmaceuticalsThe Host
Julie Rovner
KFF Health News
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
After all-night markups, two key House committees approved GOP budget legislation that would cut hundreds of billions of dollars from federal health programs over the next decade, mostly from the Medicaid program for people with low incomes or disabilities. The legislation is far from a done deal, though, with at least one Republican senator voicing opposition to Medicaid cuts.
Meanwhile, Health and Human Services Secretary Robert F. Kennedy Jr. testified before Congress for the first time since taking office. In sometimes surprisingly combative exchanges with lawmakers in the House and Senate, Kennedy denied cutting programs despite evidence to the contrary and said at one point that he doesn’t think Americans “should be taking medical advice from me.”
This week’s panelists are Julie Rovner of KFF Health News, Julie Appleby of KFF Health News, Joanne Kenen of the Johns Hopkins University Bloomberg School of Public Health and Politico Magazine, and Alice Miranda Ollstein of Politico.
Panelists
Julie Appleby
KFF Health News
Joanne Kenen
Johns Hopkins University and Politico
Alice Miranda Ollstein
Politico
Among the takeaways from this week’s episode:
- House Republicans this week released — then quickly ushered through committee — major legislation that would make deep cuts to federal spending while funding President Donald Trump’s domestic priorities, including renewing tax cuts and boosting border security. A preliminary estimate by the Congressional Budget Office found the bill would cut at least $715 billion from federal health spending over 10 years — with most of that money coming from the Medicaid program.
- Overall, the House GOP’s proposal would make it harder to enroll, and stay enrolled, in Medicaid and Affordable Care Act coverage. Among other changes, the bill would impose a requirement that nondisabled adults (with some exceptions) work, volunteer, or study at least 80 hours per month to be eligible for coverage. But Democrats and patient advocates point to evidence that, rather than encouraging employment, such a mandate results in more people losing or dropping coverage under burdensome paperwork requirements.
- Republicans also declined to extend the enhanced tax credits introduced during the covid-19 pandemic that help many people afford ACA marketplace coverage. Those tax credits expire at the end of the year, and premiums are expected to balloon, which could prompt many people not to renew their coverage.
- And Kennedy’s appearances on Capitol Hill this week provided Congress the first opportunity to question the health secretary since he assumed his post. He was grilled by Democrats about vaccines, congressionally appropriated funds, agency firings, and much more.
Plus, for “extra credit,” the panelists suggest health policy stories they read this week that they think you should read, too:
Julie Rovner: The New York Times’ “Elizabeth Holmes’s Partner Has a New Blood-Testing Start-Up,” by Rob Copeland.
Alice Miranda Ollstein: ProPublica’s “He Became the Face of Georgia’s Medicaid Work Requirement. Now He’s Fed Up With It.” by Margaret Coker, The Current.
Julie Appleby: Scientific American’s “How Trump’s National Weather Service Cuts Could Cost Lives,” by Andrea Thompson.
Joanne Kenen: The Atlantic’s “Now Is Not the Time To Eat Bagged Lettuce,” by Nicholas Florko.
Also mentioned in this week’s podcast:
- Politico’s “‘Rolling Thunder’: Inside Conservatives’ Strategy To Curb Abortion Pill Access,” by Alice Miranda Ollstein.
- The New York Times’ “Josh Hawley: Don’t Cut Medicaid,” by Sen. Josh Hawley (R-Mo.).
- NPR’s “FDA Moves To Ban Fluoride Supplements for Kids, Removing a Key Tool for Dentists,” by Pien Huang.
click to open the transcript
Transcript: GOP Poised To Cut Billions in Health Benefits
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello and welcome back to “What the Health?” I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Thursday, May 15, at 9:30 a.m. As always, and particularly this week, news happens fast and things might have changed by the time you hear this. So, here we go.
Today we are joined via videoconference by Alice Miranda Ollstein of Politico.
Alice Miranda Ollstein: Hello.
Rovner: Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico.
Joanne Kenen: Hi, everybody.
Rovner: And my KFF Health News colleague Julie Appleby.
Julie Appleby: Hi.
Rovner: No interview this week because so much news, so we will get straight to it. So, quiet week, huh? Just kidding. The House Ways and Means and Energy and Commerce committees completed all-nighter markups on their portions of President [Donald] Trump’s “one big, beautiful” reconciliation bill. And in fact, Ways and Means is officially calling it the “One, Big, Beautiful Bill” in its summary of the measure.
We will start with Energy and Commerce, which after a 26-hour marathon, one hour short of the record it set in 2017, voted out its part of the bill Wednesday afternoon, including an estimated $715 billion in reductions to health programs, mostly Medicaid, over the next 10 years. Now, the final committee bill does not include the threatened cuts to the 90% match for the Affordable Care Act expansion population, nor does it include the per capita cap for that population.
Nonetheless, it would represent the biggest cut to Medicaid in the program’s 60-year history. Guys, tell us some of the things that it would do instead to get to that $715 billion amount.
Kenen: The 715 includes some ACA cuts as well. It’s not 100% Medicaid, but it’s largely Medicaid. The biggest one is the one that we knew was almost inevitable given the current Congress, which is work requirements. It is something the Republicans have wanted a long time. In the prior administration, a few states did pass them. Arkansas got going with them. The courts stopped it.
The Medicaid statute is pretty clear that it’s about health, not about health for working people. The courts today are different. If I had to guess, I would guess there will be a legal battle and that the courts are likely to uphold work requirements.
Rovner: We’ll talk more about work requirements in a minute. But what else is in the bill?
Kenen: There’s lots of extra layers of verification. Supposedly, it’s about fraud. We can get to the Kennedy testimony later, but there were some assertions that did not add up for me. The biggest thing is work requirements, and there’s other things that will make it harder to maintain coverage, that it’s not that tou’re getting kicked off, per se. And there are also some copays. There are some copays for the upper rank. There’s been a lot of information this week. And if I get any details wrong, because we’ve all had to absorb a lot in 48 hours, someone correct me. But my recollection was a $35 copay for certain treatments for the people who are on the higher end of the income.
Rovner: Right, meaning over 100% of poverty—
Kenen: Right.
Rovner: —but still under the level required to qualify for Medicaid.
Appleby: Right. It would require states actually to impose these cost sharings of up to $35 per service. Although they’re excluding some things like primary care, emergency stuff, that kind of thing, for people in that 100% of poverty to 138% of poverty, and there’s also an upper limit of 5% of the family’s income. But that’s a lot for people in that category.
Rovner: And we know, there is an enormous body of research that says when you put copays on services, people get fewer of them. And it’s not like people who are just scraping by have a lot of extra money to spend. So we know that one of the ways that they’ll save money is that people won’t get services, presumably needed services.
Kenen: Although the primary care exemption is important, because primary care, which also usually includes pediatricians, are considered primary care, can deal with a lot of diseases that you don’t always need to see a specialist. I’m not saying it’s a good idea. I’m just saying in terms of an incentive to get basic care, keeping primary care free is an important distinction.
Rovner: Well, I do want to talk a little bit about that work requirement, which Massachusetts Democratic Rep. Jake Auchincloss called not a work requirement but a paperwork requirement. Once more, for those who haven’t heard us explain this 100 times, it’s not just people who don’t work who lose coverage because of this. I see you nodding, Alice. Please explain this again.
Ollstein: Yes. So Democrats really hammered over the course of this 26-hour hearing that the only states that have made a foray in this direction so far, Arkansas and Georgia, have seen that these work requirements do not boost employment. They kick people off who should have been eligible because they can’t navigate, like you said, the paperwork. And so it was really striking, over this hearing, where — I watched from 8 a.m. Wednesday to 2 p.m. Wednesday — and during that whole time, every single amendment vote was party-line. Nobody crossed in either direction. So this was really a political exercise in Democrats because they were not able to convince Republicans to change or soften the bill at all. They really focused on branding it, branding it as punishing the poor and threatening their health care.
And so they were pointing to what happened in Arkansas, what happened in Georgia, where the work requirements really were successful in only that they cut people from the rolls and saved the states money, not successful in helping people find work or helping people get coverage. They also made an effort to brand the copays issue. I heard Democrats calling it a “sick tax.” We’ll see if that phrase sticks around throughout this process.
Rovner: So kind of in an interesting twist, the work requirements in the bill don’t become mandatory until the year 2029. That suggests to me that those who voted for this don’t really want it to take effect, but they do want to be able to count the savings to pay for other things in the bill. And then, cherry on top of the sundae, if Democrats want to repeal the work requirements later, they would have to find a way to pay for them, because the savings would get built into the budget baseline. Or is that just me being cynical because I’ve only had like five hours of sleep this week?
Kenen: Well, there are two important dates between now and 2029. One is the 2026 off-year elections, the House elections and some Senate, and then 2028 is the presidential. So there’s several things that have changed politically about Medicaid in recent years, which we can talk to and which I’ve written about quite extensively. One of them is that a lot of people who are Trump’s base are now on Medicaid and particularly that expansion population, and nobody likes having their health care taken away from them, particularly if it’s free or very, very heavily subsidized in the lower ranks of the exchanges.
So if you’re going to kick your own voters off of their health care, you’re probably more likely to want to do it after they voted for you again. It is not uniquely cynical. We have seen both parties do similar things over the years, either for budgetary game-playing or for political things. It’s quite notable that this goes into effect in 2029.
Ollstein: It’s just interesting that this is getting criticized from both sides. So Democrats are upset that Republicans want to reap the nominal savings but not have to look like the bad guy. And conservative Republicans are upset that this doesn’t kick in sooner, because they want stricter work requirements even sooner to cut the program even more. So it’s pleasing few.
Rovner: Well, as Joanne alluded to, it’s not just Medicaid. This bill is also a bit of a stealth assault on the Affordable Care Act, too. Right, Julie? We haven’t talked about it a lot, but this administration seems to be working very hard to make the ACA a lot less effective. And the combination of reductions in Medicaid and changes to the ACA will mean lots more people will be uninsured if this bill becomes law in its current form. Yes?
Appleby: There are a lot of moving parts to this. So yeah, let’s back up just briefly and look at March, when the Trump administration did propose their first major rule affecting the Affordable Care Act, and it’s called the Patient Protection and Affordable Care Act; Marketplace Integrity … it’s a long-name rule. Anyway, it does a bunch of things. For one, it shortens the open enrollment period by about a month. So open enrollment would end on Dec. 15. And notably, this would apply to all states that run their own state-based marketplaces, as well as the federal marketplace. So there’s 16 plus D.C. that do that. So they would all also be tied to this. So that’s one of the things that the rule would do if it’s finalized in its form.
It would also end a special enrollment period that allows low-income people to essentially enroll anytime during the year. And people who are automatically reenrolled in a zero-premium plan would instead be charged a $5 premium for reenrollment in that same plan until they confirm their eligibility. Now, the Trump administration says that a lot of these rules are in part to try to combat what they say is fraud and waste, and they point to situations where people are being enrolled without their permission or switched to different plans, generally these zero-premium plans, by unscrupulous brokers who are trying to get commissions.
We’ve written a lot about that over the past year. So they’re saying that, Oh, we need to do this so that people know they’ve been enrolled. The special enrollment period for low-income people they thought was part of that. That’s disputed by a number of places. And some of the states have pushed back on this, too, and said, Hey, we don’t have this problem with fraud, so why would this now apply to us? Why would the special enrollment period, the shortened enrollment period, etc., etc.?
So those are things in the proposed rule. And the proposed rule acknowledges that it would reduce enrollment by about up to 2 million people in 2026, with coverage losses concentrated in a bunch of states like Alabama, Florida, Georgia, etc. So that’s the proposed rule. And then if you look at the House bill, like, for example, Energy and Commerce, these would codify some of those proposals from that ACA rule. So it would make it harder for a future president to change the rule and that kind of thing.
So those things that are codified would be — there’d be more hoops to jump through to verify income, for one thing. That special enrollment period based on income would be barred, and the shorter enrollment period would be in it. And if this goes through, these changes are set to go into effect next year. So a lot of insurers and states would have to scramble to try to get this put in place by then. So that’s just a short thing about what some of the ACA effects would be.
Rovner: So, it feels like there’s kind of a theme here that’s going to make it harder for people to get on and stay on both the ACA and Medicaid. Is that sort of a fair way to describe this?
Appleby: Yeah, that’s fair. In the House bills, there are also a lot of things that would bar automatic reenrollment, which a lot of people rely on. People just don’t go back in and sign up for their coverage. They’re automatically reenrolled. The bills differ a little bit. The harshest one would require everybody to sort of verify their income before they can reenroll. There would be a lot more of that. So it would essentially bar reenrollment. And we haven’t even talked about the enhanced tax credits, because that’s also sort of fitting here.
Rovner: Which was my, yes, my next question. So there’s been a lot of fighting this week about how many people would lose coverage as a result of this bill, and a lot of it is sort of philosophical fighting. We don’t have final CBO [Congressional Budget Office] numbers yet. We may not have them for another week, I am told. But what we do know is one of the things this bill could do but doesn’t do is re-up those additional subsidies that were installed during the Biden administration, during covid, that basically effectively doubled the number of people who enrolled under the marketplaces, right?
Appleby: It certainly added a lot. Most people who get a subsidy are benefiting from the enhanced subsidies. And remember, these sort of expanded at the lower end and it cut off that cliff at 400% of the poverty level that used to exist where you wouldn’t get a subsidy if you made more than that. So it smoothed all that out. So a lot of people are getting these extra subsidies.
And a lot of the data I’ve seen have said — I’m looking at an Oliver Wyman report earlier — something like, if these enhanced subsidies are allowed to expire at the end of this year, which they’re poised to do unless Congress acts, that, on average, premiums would go up by about 90%. That will be enough to cause a lot of people not to reenroll. So that’s where we’ve seen some of these estimates of I think it’s around 5 million people may not reenroll as a result of that over time.
That’s a pretty big number. But like you said, there’s a lot of numbers in the mix, but the enhanced premium subsidies do cost taxpayers. It’s not inexpensive. So if they’re looking for savings, which they are, Congress may decide not to extend them. But at the same time, many people and in a lot of states that are dominated by the GOP and others, people are getting these subsidies, and it would suddenly be a huge hit to many people to have a 90% increase in their premiums, for example.
Rovner: Yeah, as Joanne said. Which you’re about to say again, right? These are Republican voters now, right?
Kenen: I think that’s more mixed, the upper income within the ACA. We’ve expected that to go away, because there’s a difference between Congress having to yank something away versus something in the law that expires and they have to proactively renew it. We have always anticipated that enhanced subsidies would decline this year. But I just sort of want to point out, during the first Trump administration, without all this coverage, the uninsurance rate rose in the country.
And that even before ’29, there are all sorts of things, with shortened enrollment periods, how much outreach they do, there’s lots of things even before 2029 that we can expect a fairly significant erosion of health coverage. Not to what it was in pre-ACA levels — it’s not going to be that extreme, and not all the benefits that those of us with employer-sponsored insurance also get, some things through the ACA.
So this is not repeal — it’s damage. And it’s more damage than they did in the first Trump administration. All of us would be extremely surprised if there was not a significant drop in the number of insured Americans one, two years from now.
Rovner: One of the ways conservatives hope to secure the votes for this bill in the House is a provision that would bar Planned Parenthood from the Medicaid program. This would certainly be popular in the House. But when it was in the Affordable Care Act repeal bill in 2017, the Senate parliamentarian ruled that it couldn’t be included in budget reconciliation, because it is not primarily budgetary. Alice, are House leaders just hoping no one will remember that?
Ollstein: If at first you don’t succeed, try, try again. Yes, I think so. And especially because we just got a new CBO estimate of what the budgetary impact of cutting these funds would be. And it’s, like they have found before, it does not save money. It actually costs the government money because people lose access to contraception and don’t have other sources that they can afford to obtain contraception. And it’s a lot more expensive to have a baby on Medicaid than to access contraception. So I think that also contributes to the parliamentarian problem.
Rovner: Yes. You can put stuff in reconciliation that costs money, but that was sort of not the intent here. Joanne, you wanted to say something.
Kenen: And we should point out that this is still at the committee level, right? Is it going to get through the House in this exact form? We can’t be sure yet. Is something going to get through the House at the end of the day? Yes. Yes. But is all of this going to get in? Is this the final draft? Probably not. You have moderates who are still, don’t like some of the things in here, and you have conservatives who think it doesn’t go far enough.
As we said at the beginning, as far as it does go, it does not go anywhere near as far as the initial, of some of the things that were being discussed, which really would have ended Medicaid as an entitlement. These are big changes. They’re not existential in the same way that a per capita cap or a block grant or blowing up the ACA expansion by changing the rates. There are things they could have done that were far more radical that they don’t have the votes for. And—
Rovner: But they still can only lose, what, three or four votes and get something through the House.
Kenen: Right. Right. Because Medicaid is actually quite popular, and people in both parties are covered by it. We still don’t know the pathway, what gets through the House at the end of the day. Something does, right? We all think that they will, somehow or other. Not necessarily by Memorial Day, right? But something at some point will get through the House, and we don’t know exactly what it looks like.
Rovner: For the record, I’m still shrugging. I think something gets—
Kenen: And it is a bigger question mark, you know?
Rovner: Which is my next question. What are the prospects for this bill in the Senate? Do we really believe that the very conservative Missouri Republican Josh Hawley would vote against this? He had a piece in The New York Times this week saying, “Don’t Cut Medicaid.”
Kenen: He’s been really consistent. Have we seen politicians do huge flip-flops in our years of covering Congress and politics? Yes. He’s really out there on this. It’s sort of hard to see how he just says, Whoops, I didn’t really mean it. But right now in terms of who’s out there in public, we don’t have a critical mass of people who’ve said they can’t vote for this. But we do know there are provisions in this very extensive bill that some people don’t like. It will go through changes in the Senate.
I don’t have a grasp and I don’t think any of us have a grasp on exactly what’s going to change. I think work requirements, depending on what bells and whistles are attached, could get through the Senate. There might be changes like making it a state option or redefining certain things with it. I think there probably are 51 votes for a work requirement of some type in the Senate.
That doesn’t mean the way this has been written survives. And there’s just — these are big cuts. And there’s also, remember, we’re only talking about the health stuff. There’s a lot. There’s energy. There’s all sorts of — this is a big bill. This is a big, historic bill. There’s lots and lots of hurdles. We all remember that the ACA repeal, it took several tries. It was really harder than expected. It finally got through the House, and it did die in the Senate. So this is not the last word. We don’t have to shut the podcast.
Rovner: Yes, long way to go. All right, moving on. Health and Human Services Secretary Robert F. Kennedy Jr. testified before not one but two committees on Wednesday: the House labor, HHS Appropriations subcommittee in the morning and the Senate Health, Education, Labor, and Pensions Committee in the afternoon. And shall we say it didn’t all go swimmingly. Right off the bat, this was the greeting he got from House Appropriations Committee ranking member Rosa DeLauro of Connecticut. DeLauro basically saying, Everything you’re doing is illegal.
Rep. Rosa DeLauro: Mr. Secretary, this administration is recklessly and unlawfully freezing and stealing congressionally appropriated funds from a wide swath of agencies, programs, and services across the government that serve the American people. And recall that this is a violation of the Constitution.
The power of the purse resides with the Congress. It’s Article 1, Section 9, Clause 7. Yourself and President Trump and Elon Musk are attacking health programs to pay for tax cuts for billionaires. And by promoting quackery, we are endangering the health of the American people with pseudoscience, fearmongering, and misinformation.
Rovner: If you want to hear more, we did a live recap of the hearings yesterday afternoon. You can find that on KFF’s YouTube page. But I want to know what you all took away from the hearings. Joanne, you watched most of them, right?
Kenen: I watched a lot of it. I did not watch every minute of both hearings, but I watched enough. And I thought that very first exchange with DeLauro was really striking because she kept saying, over and over and over again she kept saying: Congress appropriated this money. You don’t have the right to not spend it. And he kept saying, If you appropriate the money, I will spend it. And she said, We have appropriated the money, and you’re not spending it. And he said, If you appropriate the money …
And she explained. What a continuing wrestle. It was like this endless — well, it wasn’t endless, but it was repeated when she kept saying, We appropriated it, and he kept saying, Huh? And she actually said the first time sort of under her breath, but the mic picked it up, and then she said it again. She said, “Unbelievable.” She’s not known for understatement, but she said, “Unbelievable.” And then she said it again. “Unbelievable.” So that was sort of — the rest of the day was sort of there.
Rovner: Yeah. I personally found it refreshing that someone finally called out HHS, saying: You know, there was an appropriations bill that got signed by the president, and you are withholding this money. And this is our province. We get to decide how the money is spent. You don’t get to decide how the money is spent. The other big headline that came out of this hearing was when Kennedy said that, after being raked over the coals again about his vaccine comments, he said, Well, you shouldn’t be taking medical advice from me. And I’m like, isn’t that the job of the HHS secretary?
Ollstein: It was very clear that, like in the markups of the bill, Democrats, unless Republicans are willing to cross the aisle and join them, are just left sort of railing against what’s happening and not really having any power to impact it. We did see some Republicans expressing some concern about the cuts that have happened. But unless that turns into real oversight action, real legislative action, I just imagine we’re set up for this to happen again where Congress appropriates and the cuts happen anyway.
Rovner: I was surprised at how much Sen. Cassidy, Sen. Bill Cassidy, the chairman of the HELP Committee, didn’t say. He basically said when he voted for Kennedy’s nomination that he was torn. He believes in vaccines. He’s a practicing doctor. He, Cassidy. And he made Kennedy promise that he wasn’t going to change any of these vaccine rules, which he’s already done. And he’s installed anti-vax people at many levels of HHS. And yet Cassidy was incredibly conciliatory in his opening statement.
And it was left to Chris Murphy of all people, the firebrand Democrat from Connecticut, to basically be Cassidy’s anger manager. And sort of, he said, “If I were the chairman … my head would be exploding,” which I believe is a line that I’ve been saying for the last several months. What’s happening with Cassidy? Do we know? He can’t be happy with what’s happening here.
Ollstein: This was well previewed by everything Cassidy has sort of put out publicly since the confirmation hearing. If you track his press releases, they’ve been sort of selectively praising HHS for doing certain things and being silent on the things that we imagine he might not like on the vaccine front. And so that dynamic carried forward right into this hearing, which was the first opportunity for Congress to really grill Kennedy since he’s taken office.
And so many people have pointed out that Cassidy is up for reelection. He is facing a primary challenge from the right. He wants to align himself with the Trump administration and with the sort of “MAGA [Make America great Again]” movement. And he has pushed back on accusations that his treatment of Kennedy is influenced by that, but people can draw their own conclusions.
Kenen: I also wanted to point out that Kennedy insisted that he hadn’t fired any scientists, and he made that assertion a few times, which I think the Democrats, their jaws collectively dropped in unison. The cuts to NIH [the National Institutes of Health] have been extreme, in the billions. And in addition to the NIH scientists, there are also the ripple effect of training the next generation of scientists, because of the cuts to universities.
And also Kennedy, I sort of noticed at one point he was saying something about some universities don’t need this money, but then he mentioned specifically but Maine, where Susan Collins is the chair of the Appropriations Committee of the Senate, and Alabama, where Katie Britt has been, Sen. Katie Britt, has been sort of vocal about this, which is also, people don’t think of or may not realize that University of Alabama is a huge scientific center.
It is a powerhouse, but it is a state-funded university without such a big environment. Kennedy said: You know what? We’re going to make these cuts. But maybe not Maine and Alabama. It was like — talk about politics. But I think that they were really floored when he said over and over again that no scientists have been let go.
Rovner: You were right. There was also a lot of sort of ad hoc, If you have a particular problem, why don’t you—
Kenen: Call my office.
Rovner: —call my office. Yeah. And we can take care of it. Which seemed just sort of mind-blowing to me. It’s like, this is how we’re making policy now. And somebody, I meant to go back and look at who, somebody in the morning at the House hearing, one of the Democrats, said, Is there a special phone number for Democrats to call your office to see if we can get some of these cuts restored? That literally seems to be how HHS is being run right now.
Ollstein: And I think it’s reflected across the government. When Elon Musk was more involved directly with the DOGE [Department of Government Efficiency] stuff, he was reportedly telling Republican senators the same. Oh, if you have an issue, you know, just text me, just call me. And folks who study government pointed out that this smacks of the kind of personalism that has defined some authoritarian governments in the past where things happen more through favors than through normal government processes that are more transparent.
Kenen: And a phone call from your senator is not how you should be able to get back into a clinical trial. There was also a lot of exchanges about what’s happening to clinical trials and harm to patients, which he was — there was some gaps there. And you’re watching him saying, Oh yeah, I can get her in. Just, you call me tomorrow. Call my office, to Sen. [Patty] Murray. And the state of him asserting that not much has changed and anything we got wrong we’ll fix versus the fact that huge numbers of things have changed that have affected both patients and future patients.
One of the Democrats said: What’s wrong with researching cancer and Alzheimer’s, particularly if you’re trying to deal with chronic diseases? These are chronic conditions, and we’re gutting research into them. So there was a lot of disconnects. There was some, also—
Rovner: It’s not just cuts. They are pushing the “Make America Healthy Again” agenda. Just this week the FDA [Food and Drug Administration] is moving to ban fluoride supplements for kids. These are generally drops, tablets, and lozenges prescribed to kids who live in places that don’t have fluoridated water.
This move contradicts recommendations from both the CDC [Centers for Disease Control and Prevention] and the U.S. Preventive Health Services Task Force. And RFK was taken to task at the House hearing by Congressman Mike Simpson of Idaho, who’s one of a handful of dentists in the chamber. I have to say I didn’t have eliminating fluoride on my 2025 public health bingo card.
Ollstein: Yes. And I think that this is raising concerns for a few reasons. One, the public health impact. This goes against decades of research and evidence and the medical community’s consensus. But this also is moving sort of beyond the personal-choice, medical freedom kind of framing that has been used to argue about fluoridating public water. This is taking away a parent’s choice, potentially. If they want these supplements for their kids, they’re not going to be available any longer. And this is exactly what people fear could extend into the vaccine space. It’s not just that it’s going to not have mandates for schools or rules around that, that it won’t even be an option for the people who want it.
Rovner: All right, well, moving on to abortion, the one piece of potential news out of the Kennedy hearings came in response to a question from the aforementioned Sen. Josh Hawley from Missouri about a new study claiming that the abortion pill mifepristone has way more complications than numerous studies over the past 40 years it’s been in use have found. Alice, tell us about this particular study, which RFK Jr. suggested might prompt the FDA to change the status of the abortion pill.
Ollstein: So, one, it’s not a study. Even its supporters admit in private that it’s not a study. I obtained a private conversation that a lot of these groups pushing this held recently to talk about how they hoped to use this information to influence government policy. And they noted that because this is something that a conservative think tank just put out themselves, they did not submit it to a medical journal. It did not go through peer review.
So they said directly that it is not a study in the traditional sense. Still, you have senators and now the secretary of health and human services referring to it as a study and calling for policy changes based on it. So I want people to keep that in mind as this is discussed going forward. These drugs have been available for 25 years now. There have been lots of more rigorous, peer-reviewed studies that have found them to be overwhelmingly safe and effective.
Some of this new data actually aligns with some of the findings from those previous, more rigorous studies, but their own unique definitions of certain things, calling some things adverse events when the FDA does not consider that to be so, and so medical experts told me, including some from KFF, that this has so many red flags that they think it could never have been published in a credible medical journal.
Rovner: And just to clarify, while we’re talking about different time periods: It’s been available in the U.S. for 25 years.
Ollstein: Yes.
Rovner: It’s been available internationally since the 1980s.
Ollstein: Right. Right.
Rovner: So, it has been well studied for quite a long time. Well, in other abortion news this week, the Texas Legislature is moving forward with a new piece of anti-abortion legislation that can’t be challenged in court, this one aimed at the abortion pill. Alice, this is like Chapter 2 in Texas trying to figure out how they can ban abortion-related things without anybody challenging the law, right?
Ollstein: There’s a lot of different moving parts right now. There’s that. There’s the new case that’s also pending in Texas, brought by three GOP states seeking to impose national restrictions on abortion pills. There’s this new review that the FDA is allegedly going to undertake around dispensing rules. And so this has been an overwhelming focus of the anti-abortion movement since even before Dobbs, but especially now.
They know that the ability of people to get these pills prescribed online, sent by mail, is the primary way that people are getting around state bans, other than travel, which is not always possible for folks. And so there are just efforts going on in state legislatures, in Congress, in the FDA, in state courts and federal courts, all to impose restrictions.
And so it’s a very throw-spaghetti-at-the-wall-and-see-what-sticks approach. But that has proven very effective for them over the decades. Arguably that’s how we got to where we are now, where abortion is banned in much of the country. So it’s something to take seriously and watch carefully.
Rovner: And this is Texas trying again with this. Individuals can sue other individuals who they think have used the abortion pill. It does not require the involvement of the state to prosecute, which has not, I don’t think, spread beyond Texas at this point, but it would be Texas’ second bite at this apple.
Kenen: But the proposed language in that bill is extraordinary. We at the state legislature of Texas is passing a bill and no court has the right to review whether it is constitutional, etc. It seems pretty extreme, right?
Rovner: Well, this was how Texas did their first ban.
Kenen: Right.
Rovner: Remember that the Supreme Court allowed it to stand because they weren’t quite sure what to do with it.
Kenen: But that was also because they did unique legal things in terms of, they sort of created a legal structure. This, the language is in the bill — and no court can double-check us.
Rovner: Yeah.
Kenen: So, and then what else can they use that for, right? And apparently there are even some Republicans who are a little concerned about that language. And I’m not up on the exact makeup of constitutional views of the entire Texas Legislature.
Rovner: Yes. We should point out, it hasn’t passed the full legislature yet.
Kenen: No. It’s proposed.
Rovner: Just the Texas Senate. It’s passed the Senate. We’re awaiting to see if it will pass the Texas House. All right, well, finally in this incredibly newsy week, just before he left for his overseas trip, President Trump unveiled what he touted as an enormous announcement that turned out to be an executive order basically wishing down drug prices by tying them to other countries’ price-controlled prices. Except this isn’t really going to happen anytime soon. Right, Julie?
Appleby: Well, it is interesting. It’s this “most favored nations” idea that we would tie drug prices in the United States to what’s paid by other countries where they have much stronger drug negotiation issues. And it’s not clear how it works. So yeah, it’s not clear what the path forward is with that.
Ollstein: The problem with saying drug prices are coming down is if they do not come down, people might be mad at you for saying they’re coming down.
Rovner: I would say he did wish down the price of eggs. He said that egg prices were coming down when they weren’t, except now they are, because he had nothing to do with them going up or coming down. It had to do with the bird flu. And so now he can say, See, I got egg prices down.
Kenen: But they’re still higher than they were when he—
Rovner: They are still higher than they were.
Kenen: But they have come down.
Rovner: But I will say, I was going to say, this is super-clever marketing. This is the one thing that President Trump is really, really good at. He hyped this announcement ahead of time. He actually got headlines insisting that this will really do something. I have had people tell me that they’ve had sort of their grown kids and stuff saying: Oh look, drug prices. He’s going to reduce drug prices. When in fact this is one of those executive orders that just doesn’t really do anything.
Kenen: We don’t know what’s going to happen to drug prices over the next four years. There’s a law on the books from the Biden administration. In his first administration, I think it might’ve even been a day or two before inauguration, he went on a tear against the drug companies. Remember, he called them killers or something like that. And he also came up with a list of something like 40-odd steps that he could take. And I think half of them had a question mark after them. So he’s been mad at drug prices for a while now. He did not achieve that in the first administration. That’s bipartisan. There’s no Americans who want to pay higher prices for drugs, unless maybe they work for a drug company. People want more—
Rovner: Right. It’s an 80/20 issue — 80% of people want drug prices down.
Kenen: Right.
Rovner: That’s probably more than an 80/20 issue.
Kenen: There could be some room for bipartisanship on drugs. There’s not a lot of room for bipartisanship, but that’s particularly if he’s not trying to repeal what [President Joe] Biden did, if that stays or gets built on. We don’t know what’s going to happen. But no, you can’t just sign an executive order. It’s not a magic wand.
Rovner: And I don’t think we’re going to be importing other countries’ price controls anytime soon. I’m going to go on a limb on that one. All right, that is this week’s news. Now it is time for our extra-credit segment. That’s where we each recognize a story we read this week we think you should read, too. Don’t worry if you miss it. We’ll put the links in our show notes on your phone or other mobile device. Alice, I want you to go first this week because you have a story that’s directly relevant to something that we talked about in the Medicaid discussion.
Ollstein: Yeah. So I have this great story from ProPublica [“He Became the Face of Georgia’s Medicaid Work Requirement. Now He’s Fed Up With It.”] about Medicaid work requirements and about how the small-business owner that Georgia decided to make the face of its program, and they filmed a video of him praising it, even he multiple times lost his coverage, even though he tried to do everything right. He logged his work hours. He signed up for alerts. And just because of bureaucratic things and falling through the cracks, two times he lost his coverage and he had to plead for someone to intervene to get him his benefits back. And he has really soured on all of this, even though he was the face of selling it that the governor used. So I think this is a great example of what could happen as this is debated as a national policy.
Rovner: And I will say, I learned about this ProPublica story from the markup, where a number of members brought it up. He’s now the poster child for what happens when you have work requirements, even if people are working. Joanne.
Kenen: There’s a great piece in The Atlantic by Nick Florko called “Now Is Not the Time To Eat Bagged Lettuce.” And although it is not in the headline, it’s particularly romaine, which has periodically been in the news as being a source of harmful bacteria. And if you think you can just buy bagged lettuce and wash it yourself and it’ll be safe — no, that doesn’t work, either.
Basically it goes through like the equivalent of a salad woodchopper and there are all this different lettuce. All this lettuce goes through it. And once one blade gets contaminated, it all gets contaminated. So also, if you are a part of a marriage or one of you likes romaine and the other one would rather have red leaf, this is pretty good ammunition, right? But we should be going back to buying heads of lettuce, washing them yourself.
And they’re not as safe and sanitary as it sounds, particularly as some issues are going on right now. And of course, we have less public notification and less monitoring and there’s less, less, less of food safety kinds of things coming down the pike at FDA. So it’s even more timely.
Rovner: It’s a pretty vivid story. Julie.
Appleby: Thanks. Mine is also, the story I’ve picked is also along the same lines of cuts and what the perhaps unintended consequences were, but the consequences nonetheless. And it’s from the Scientific American. It’s by Andrea Thompson. The headline is “How Trump’s National Weather Service Cuts Could Cost Lives.”
And it just talks about the National Weather Service with a lot of interesting facts that I didn’t know for sure, that how the improvements have been made in forecasting, why this is important, and how it’s understaffed, and how these cuts are going to just make things worse. And it talks about it costs the average American, it says, about $4 a year for the National Weather Service. “It’s a cup of coffee,” said one person that’s being quoted.
And it said the National Weather Service provides an overall benefit of $100 billion to the economy. Aside from the fact that you might want a tornado warning ahead of time, that kind of thing, this is also just really important to quantify the overall value at a time when we are seeing a lot of hurricanes and tornadoes and other climate issues going on. So that would be my pick.
Kenen: But the Sharpie can just make it move.
Rovner: Yeah, that’s true. All right, my extra credit this week is what Joanne has dubbed “Theranos for Pets,” though the actual headline in The New York Times is “Elizabeth Holmes’s Partner Has a New Blood-Testing Start-Up.” And it’s kind of a scary history-repeats-itself story. Even as Elizabeth Holmes herself remains in jail, having been convicted of fraud over her novel blood-testing company that was really cool but also didn’t work, her partner and the father of her two children, Billy Evans, is raising money for a new blood-testing company.
He’s called it Haemanthus — I hope I’ve said that right — which is a flower also called the blood lily. And unlike his incarcerated partner, Evans plans to start out by testing the blood of pets, then move to humans. As they say, what could possibly go wrong?
All right, that is this week’s show. As always, if you enjoy the podcast, you can subscribe wherever you get your podcasts. We’d appreciate it if you left us a review. That helps other people find us, too. Thanks as always to our editor, Emmarie Huetteman, and our producer, Francis Yang. Also, as always, you can email us your comments or questions. We’re at whatthehealth@kff.org. Or you can still find me on X, @jrovner, or on Bluesky, @julierovner. Where are you guys hanging these days? Julie Appleby.
Appleby: I’m still on X, @Julie_appleby.
Rovner: Joanne.
Kenen: I’m only a little on X. I’m more on Bluesky and LinkedIn, @joannekenen.
Rovner: Alice.
Ollstein: Mostly on Bluesky, @alicemiranda, and still on X, @AliceOllstein.
Rovner: We will be back in your feed next week. Until then, be healthy.
Credits
Francis Ying
Audio producer
Emmarie Huetteman
Editor
To hear all our podcasts, click here.
And subscribe to KFF Health News’ “What the Health?” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).

Pain Clinic CEO Faced 20 Years for Making Patients ‘Human Pin Cushions.’ He Got 18 Months.
NASHVILLE, Tenn. — Federal prosecutors sought a maximum prison sentence of nearly 20 years for the CEO of Pain MD, a company found to have given hundreds of thousands of questionable injections to patients, many reliant on opioids. It would have been among the longest […]
Pharmaceuticals
Honey, Sweetie, Dearie: The Perils of Elderspeak
A prime example of elderspeak: Cindy Smith was visiting her father in his assisted living apartment in Roseville, California. An aide who was trying to induce him to do something — Smith no longer remembers exactly what — said, “Let me help you, sweetheart.” “He […]
Pharmaceuticals KFF Health News' 'What the Health?': Cutting Medicaid Is Hard — Even for the GOP
The Host Julie Rovner KFF Health News @jrovner @julierovner.bsky.social Read Julie’s stories. Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the […]
PharmaceuticalsThe Host
Julie Rovner
KFF Health News
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, “What the Health?” A noted expert on health policy issues, Julie is the author of the critically praised reference book “Health Care Politics and Policy A to Z,” now in its third edition.
After narrowly passing a budget resolution this spring foreshadowing major Medicaid cuts, Republicans in Congress are having trouble agreeing on specific ways to save billions of dollars from a pool of funding that pays for the program without cutting benefits on which millions of Americans rely. Moderates resist changes they say would harm their constituents, while fiscal conservatives say they won’t vote for smaller cuts than those called for in the budget resolution. The fate of President Donald Trump’s “one big, beautiful bill” containing renewed tax cuts and boosted immigration enforcement could hang on a Medicaid deal.
Meanwhile, the Trump administration surprised those on both sides of the abortion debate by agreeing with the Biden administration that a Texas case challenging the FDA’s approval of the abortion pill mifepristone should be dropped. It’s clear the administration’s request is purely technical, though, and has no bearing on whether officials plan to protect the abortion pill’s availability.
This week’s panelists are Julie Rovner of KFF Health News, Anna Edney of Bloomberg News, Maya Goldman of Axios, and Sandhya Raman of CQ Roll Call.
Panelists
Anna Edney
Bloomberg News
Maya Goldman
Axios
Sandhya Raman
CQ Roll Call
Among the takeaways from this week’s episode:
- Congressional Republicans are making halting progress on negotiations over government spending cuts. As hard-line House conservatives push for deeper cuts to the Medicaid program, their GOP colleagues representing districts that heavily depend on Medicaid coverage are pushing back. House Republican leaders are eying a Memorial Day deadline, and key committees are scheduled to review the legislation next week — but first, Republicans need to agree on what that legislation says.
- Trump withdrew his nomination of Janette Nesheiwat for U.S. surgeon general amid accusations she misrepresented her academic credentials and criticism from the far right. In her place, he nominated Casey Means, a physician who is an ally of HHS Secretary Robert F. Kennedy Jr.’s and a prominent advocate of the “Make America Healthy Again” movement.
- The pharmaceutical industry is on alert as Trump prepares to sign an executive order directing agencies to look into “most-favored-nation” pricing, a policy that would set U.S. drug prices to the lowest level paid by similar countries. The president explored that policy during his first administration, and the drug industry sued to stop it. Drugmakers are already on edge over Trump’s plan to impose tariffs on drugs and their ingredients.
- And Kennedy is scheduled to appear before the Senate’s Health, Education, Labor and Pensions Committee next week. The hearing would be the first time the secretary of Health and Human Services has appeared before the HELP Committee since his confirmation hearings — and all eyes are on the committee’s GOP chairman, Sen. Bill Cassidy of Louisiana, a physician who expressed deep concerns at the time, including about Kennedy’s stances on vaccines.
Also this week, Rovner interviews KFF Health News’ Lauren Sausser, who co-reported and co-wrote the latest KFF Health News’ “Bill of the Month” installment, about an unexpected bill for what seemed like preventive care. If you have an outrageous, baffling, or infuriating medical bill you’d like to share with us, you can do that here.
Plus, for “extra credit” the panelists suggest health policy stories they read this week that they think you should read, too:
Julie Rovner: NPR’s “Fired, Rehired, and Fired Again: Some Federal Workers Find They’re Suddenly Uninsured,” by Andrea Hsu.
Maya Goldman: Stat’s “Europe Unveils $565 Million Package To Retain Scientists, and Attract New Ones,” by Andrew Joseph.
Anna Edney: Bloomberg News’ “A Former TV Writer Found a Health-Care Loophole That Threatens To Blow Up Obamacare,” by Zachary R. Mider and Zeke Faux.
Sandhya Raman: The Louisiana Illuminator’s “In the Deep South, Health Care Fights Echo Civil Rights Battles,” by Anna Claire Vollers.
Also mentioned in this week’s podcast:
- ProPublica’s series “Life of the Mother: How Abortion Bans Lead to Preventable Deaths,” by Kavitha Surana, Lizzie Presser, Cassandra Jaramillo, and Stacy Kranitz, and the winner of the 2025 Pulitzer Prize for public service journalism.
- The New York Times’ “G.O.P. Targets a Medicaid Loophole Used by 49 States To Grab Federal Money,” by Margot Sanger-Katz and Sarah Kliff.
- KFF Health News’ “Seeking Spending Cuts, GOP Lawmakers Target a Tax Hospitals Love to Pay,” by Phil Galewitz.
- Axios’ “Out-of-Pocket Drug Spending Hit $98B in 2024: Report,” by Maya Goldman.
click to open the transcript
Transcript: Cutting Medicaid Is Hard — Even for the GOP
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello and welcome back to “What the Health?” I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters in Washington. We’re taping this week on Thursday, May 8, at 10 a.m. As always, news happens fast and things might have changed by the time you hear this. So, here we go.
Today we are joined via a videoconference by Anna Edney of Bloomberg News.
Anna Edney: Hi, everybody.
Rovner: Maya Goldman of Axios News.
Maya Goldman: Great to be here.
Rovner: And Sandhya Raman of CQ Roll Call.
Sandhya Raman: Good morning, everyone.
Rovner: Later in this episode we’ll have my “Bill of the Month” interview with my KFF Health News colleague Lauren Sausser. This month’s patient got preventive care they assumed would be covered by their Affordable Care Act health plan, except it wasn’t. But first, this week’s news.
We’re going to start on Capitol Hill, where Sandhya is coming directly from, where regular listeners to this podcast will be not one bit surprised that Republicans working on President [Donald] Trump’s one “big, beautiful” budget reconciliation bill are at an impasse over how and how deeply to cut the Medicaid program. Originally, the House Energy and Commerce Committee was supposed to mark up its portion of the bill this week, but that turned out to be too optimistic. Now they’re shooting for next week, apparently Tuesday or so, they’re saying, and apparently that Memorial Day goal to finish the bill is shifting to maybe the Fourth of July? But given what’s leaking out of the closed Republican meetings on this, even that might be too soon. Where are we with these Medicaid negotiations?
Raman: I would say a lot has been happening, but also a lot has not been happening. I think that anytime we’ve gotten any little progress on knowing what exactly is at the top of the list, it gets walked back. So earlier this week we had a meeting with a lot of the moderates in Speaker [Mike] Johnson’s office and trying to get them on board with some of the things that they were hesitant about, and following the meeting, Speaker Johnson had said that two of the things that have been a little bit more contentious — changing the federal match for the expansion population and instituting per capita caps for states — were off the table. But the way that he phrased it is kind of interesting in that he said stay tuned and that it possibly could change.
And so then yesterday when we were hearing from the Energy and Commerce Committee, it seemed like these things are still on the table. And then Speaker Johnson has kind of gone back on that and said, I said it was likely. So every time we kind of have any sort of change, it’s really unclear if these things are in the mix, outside the mix. When we pulled them off the table, we had a lot of the hard-line conservatives get really upset about this because it’s not enough savings. So I think any way that you push it with such narrow margins, it’s been difficult to make any progress, even though they’ve been having a lot of meetings this week.
Rovner: One of the things that surprised me was apparently the Senate Republicans are weighing in. The Senate Republicans who aren’t even set to make Medicaid cuts under their version of the budget resolution are saying that the House needs to go further. Where did that come from?
Raman: It’s just been a difficult process to get anything across. I mean, in the House side, a lot of it has been, I think, election-driven. You see the people that are not willing to make as many concessions are in competitive districts. The people that want to go a little bit more extreme on what they’re thinking are in much more safe districts. And then in the Senate, I think there’s a lot more at play just because they have longer terms, they have more to work with. So some of the pushback has been from people that it would directly affect their states or if the governors have weighed in. But I think that there are so many things that they do want to get done, since there is much stronger agreement on some of the immigration stuff and the taxes that they want to find the savings somewhere. If they don’t find it, then the whole thing is moot.
Rovner: So meanwhile, the Congressional Budget Office at the request of Democrats is out with estimates of what some of these Medicaid options would mean for coverage, and it gives lie to some of these Republican claims that they can cut nearly a trillion dollars from Medicaid without touching benefits, right? I mean all of these — and Maya, your nodding.
Goldman: Yeah.
Rovner: All of these things would come with coverage losses.
Goldman: Yeah, I think it’s important to think about things like work requirements, which has gotten a lot of support from moderate Republicans. The only way that that produces savings is if people come off Medicaid as a result. Work requirements in and of themselves are not saving any money. So I know advocates are very concerned about any level of cuts. I talked to somebody from a nursing home association who said: We can’t pick and choose. We’re not in a position to pick and choose which are better or worse, because at this point, everything on the table is bad for us. So I think people are definitely waiting with bated breath there.
Rovner: Yeah, I’ve heard a lot of Republicans over the last week or so with the talking points. If we’re just going after fraud and abuse then we’re not going to cut anybody’s benefits. And it’s like — um, good luck with that.
Goldman: And President Trump has said that as well.
Rovner: That’s right. Well, one place Congress could recoup a lot of money from Medicaid is by cracking down on provider taxes, which 49 of the 50 states use to plump up their federal Medicaid match, if you will. Basically the state levies a tax on hospitals or nursing homes or some other group of providers, claims that money as their state share to draw down additional federal matching Medicaid funds, then returns it to the providers in the form of increased reimbursement while pocketing the difference. You can call it money laundering as some do, or creative financing as others do, or just another way to provide health care to low-income people.
But one thing it definitely is, at least right now, is legal. Congress has occasionally tried to crack down on it since the late 1980s. I have spent way more time covering this fight than I wish I had, but the combination of state and health provider pushback has always prevented it from being eliminated entirely. If you want a really good backgrounder, I point you to the excellent piece in The New York Times this week by our podcast pals Margot Sanger-Katz and Sarah Kliff. What are you guys hearing about provider taxes and other forms of state contributions and their future in all of this? Is this where they’re finally going to look to get a pot of money?
Raman: It’s still in the mix. The tricky thing is how narrow the margins are, and when you have certain moderates having a hard line saying, I don’t want to cut more than $500 billion or $600 billion, or something like that. And then you have others that don’t want to dip below the $880 billion set for the Energy and Commerce Committee. And then there are others that have said it’s not about a specific number, it’s what is being cut. So I think once we have some more numbers for some of the other things, it’ll provide a better idea of what else can fit in. Because right now for work requirements, we’re going based on some older CBO [Congressional Budget Office] numbers. We have the CBO numbers that the Democrats asked for, but it doesn’t include everything. And piecing that together is the puzzle, will illuminate some of that, if there are things that people are a little bit more on board with. But it’s still kind of soon to figure out if we’re not going to see draft text until early next week.
Goldman: I think the tricky thing with provider taxes is that it’s so baked into the way that Medicaid functions in each state. And I think I totally co-sign on the New York Times article. It was a really helpful explanation of all of this, and I would bet that you’ll see a lot of pushback from state governments, including Republicans, on a proposal that makes severe changes to that.
Rovner: Someday, but not today, I will tell the story of the 1991 fight over this in which there was basically a bizarre dealmaking with individual senators to keep this legal. That was a year when the Democrats were trying to get rid of it. So it’s a bipartisan thing. All right, well, moving on.
It wouldn’t be a Thursday morning if we didn’t have breaking federal health personnel news. Today was supposed to be the confirmation hearing for surgeon general nominee and Fox News contributor Janette Nesheiwat. But now her nomination has been pulled over some questions about whether she was misrepresenting her medical education credentials, and she’s already been replaced with the nomination of Casey Means, the sister of top [Health and Human Services] Secretary [Robert F.] Kennedy [Jr.] aide Calley Means, who are both leaders in the MAHA [“Make America Healthy Again”] movement. This feels like a lot of science deniers moving in at one time. Or is it just me?
Edney: Yeah, I think that the Meanses have been in this circle, names floated for various things at various times, and this was a place where Casey Means fit in. And certainly she espouses a lot of the views on, like, functional medicine and things that this administration, at least RFK Jr., seems to also subscribe to. But the one thing I’m not as clear on her is where she stands with vaccines, because obviously Nesheiwat had fudged on her school a little bit, and—
Rovner: Yeah, I think she did her residency at the University of Arkansas—
Edney: That’s where.
Rovner: —and she implied that she’d graduated from the University of Arkansas medical school when in fact she graduated from an accredited Caribbean medical school, which lots of doctors go to. It’s not a sin—
Edney: Right.
Rovner: —and it’s a perfectly, as I say, accredited medical school. That was basically — but she did fudge it on her resume.
Edney: Yeah.
Rovner: So apparently that was one of the things that got her pulled.
Edney: Right. And the other, kind of, that we’ve seen in recent days, again, is Laura Loomer coming out against her because she thinks she’s not anti-vaccine enough. So what the question I think to maybe be looking into today and after is: Is Casey Means anti-vaccine enough for them? I don’t know exactly the answer to that and whether she’ll make it through as well.
Rovner: Well, we also learned this week that Vinay Prasad, a controversial figure in the covid movement and even before that, has been named to head the FDA [Food and Drug Administration] Center for Biologics and Evaluation Research, making him the nation’s lead vaccine regulator, among other things. Now he does have research bona fides but is a known skeptic of things like accelerated approval of new drugs, and apparently the biotech industry, less than thrilled with this pick, Anna?
Edney: Yeah, they are quite afraid of this pick. You could see it in the stocks for a lot of vaccine companies, for some other companies particularly. He was quite vocal and quite against the covid vaccines during covid and even compared them to the Nazi regime. So we know that there could be a lot of trouble where, already, you know, FDA has said that they’re going to require placebo-controlled trials for new vaccines and imply that any update to a covid vaccine makes it a new vaccine. So this just spells more trouble for getting vaccines to market and quickly to people. He also—you mentioned accelerated approval. This is a way that the FDA uses to try to get promising medicines to people faster. There are issues with it, and people have written about the fact that they rely on what are called surrogate endpoints. So not Did you live longer? but Did your tumor shrink?
And you would think that that would make you live longer, but it actually turns out a lot of times it doesn’t. So you maybe went through a very strong medication and felt more terrible than you might have and didn’t extend your life. So there’s a lot of that discussion, and so that. There are other drugs. Like this Sarepta drug for Duchenne muscular dystrophy is a big one that Vinay Prasad has come out against, saying that should have never been approved, because it was using these kind of surrogate endpoints. So I think biotech’s pretty — thinking they’re going to have a lot tougher road ahead to bring stuff to market.
Rovner: And I should point out that over the very long term, this has been the continuing struggle at FDA. It’s like, do you protect the public but make people wait longer for drugs or do you get the drugs out and make sure that people who have no other treatments available have something available? And it’s been a constant push and pull. It’s not really been partisan. Sometimes you get one side pushing and the other side pushing back. It’s really nothing new. It’s just the sort of latest iteration of this.
Edney: Right. Yeah. This is the pendulum swing, back to the Maybe we need to be slowing it down side. It’s also interesting because there are other discussions from RFK Jr. that, like, We need to be speeding up approvals and Trump wants to speed up approvals. So I don’t know where any of this will actually come down when the rubber meets the road, I guess.
Rovner: Sandhya and Maya, I see you both nodding. Do you want to add something?
Raman: I think this was kind of a theme that I also heard this week in the — we had the Senate Finance hearing for some of the HHS [Department of Health and Human Services] nominees, and Jim O’Neill, who’s one of the nominees, that was something that was brought up by Finance ranking member Ron Wyden, that some of his past remarks when he was originally considered to be on the short list for FDA commissioner last Trump administration is that he basically said as long as it’s safe, it should go ahead regardless of efficacy. So those comments were kind of brought back again, and he’s in another hearing now, so that might come up as an issue in HELP [the Senate Committee on Health, Education, Labor and Pensions] today.
Rovner: And he’s the nominee for deputy secretary, right? Have to make sure I keep all these things straight. Maya, you wanting to add something?
Goldman: Yeah, I was just going to say, I think there is a divide between these two philosophies on pharmaceuticals, and my sense is that the selection of Prasad is kind of showing that the anti-accelerated-approval side is winning out. But I think Anna is correct that we still don’t know where it’s going to land.
Rovner: Yes, and I will point out that accelerated approval first started during AIDS when there was no treatments and basically people were storming the — literally physically storming — the FDA, demanding access to AIDS drugs, which they did finally get. But that’s where accelerated approval came from. This is not a new fight, and it will continue.
Turning to abortion, the Trump administration surprised a lot of people this week when it continued the Biden administration’s position asking for that case in Texas challenging the abortion pill to be dropped. For those who’ve forgotten, this was a case originally filed by a bunch of Texas medical providers demanding the judge overrule the FDA’s approval of the abortion pill mifepristone in the year 2000. The Supreme Court ruled the original plaintiff lacked standing to sue, but in the meantime, three states —Missouri, Idaho, and Kansas — have taken their place as plaintiffs. But now the Trump administration points out that those states have no business suing in the Northern District of Texas, which kind of seems true on its face. But we should not mistake this to think that the Trump administration now supports the current approval status of the abortion bill. Right, Sandhya?
Raman: Yeah, I think you’re exactly right. It doesn’t surprise me. If they had allowed these three states, none of which are Texas — they shouldn’t have standing. And if they did allow them to, that would open a whole new can of worms for so many other cases where the other side on so many issues could cherry-pick in the same way. And so I think, I assume, that this will come up in future cases for them and they will continue with the positions they’ve had before. But this was probably in their best interest not to in this specific one.
Rovner: Yeah. There are also those who point out that this could be a way of the administration protecting itself. If it wants to roll back or reimpose restrictions on the abortion pill, it would help prevent blue states from suing to stop that. So it serves a double purpose here, right?
Raman: Yeah. I couldn’t see them doing it another way. And even if you go through the ruling, the language they use, it’s very careful. It’s not dipping into talking fully about abortion. It’s going purely on standing. Yeah.
Rovner: There’s nothing that says, We think the abortion pill is fine the way it is. It clearly does not say that, although they did get the headlines — and I’m sure the president wanted — that makes it look like they’re towing this middle ground on abortion, which they may be but not necessarily in this case.
Well, before we move off of reproductive health, a shoutout here to the incredible work of ProPublica, which was awarded the Pulitzer Prize for public service this week for its stories on women who died due to abortion bans that prevented them from getting care for their pregnancy complications. Regular listeners of the podcast will remember that we talked about these stories as they came out last year, but I will post another link to them in the show notes today.
OK, moving on. There’s even more drug price news this week, starting with the return of, quote, “most favored nation” drug pricing. Anna, remind us what this is and why it’s controversial.
Edney: Yeah. So the idea of most favored nation, this is something President Trump has brought up before in his first administration, but it creates a basket, essentially, of different prices that nations pay. And we’re going to base ours on the lowest price that is paid for—
Rovner: We’re importing other countries’—
Edney: —prices.
Rovner: —price limits.
Edney: Yeah. Essentially, yes. We can’t import their drugs, but we can import their prices. And so the goal is to just basically piggyback off of whoever is paying the lowest price and to base ours off of that. And clearly the drug industry does not like this and, I think, has faced a number of kind of hits this week where things are looming that could really come after them. So Politico broke that news that Trump is going to sign or expected to sign an executive order that will direct his agencies to look into this most-favored-nation effort. And it feels very much like 2.0, like we were here before. And it didn’t exactly work out, obviously.
Rovner: They sued, didn’t they? The drug industry sued, as I recall.
Edney: Yeah, I think you’re right. Yes.
Goldman: If I’m remembering—
Rovner: But I think they won.
Goldman: If I’m remembering correctly, it was an Administrative Procedure Act lawsuit though, right? So—
Rovner: It was. Yes. It was about a regulation. Yes.
Goldman: —who knows what would happen if they go through a different procedure this time.
Rovner: So the other thing, obviously, that the drug industry is freaked out about right now are tariffs, which have been on again, off again, on again, off again. Where are we with tariffs on — and it’s not just tariffs on drugs being imported. It’s tariffs on drug ingredients being imported, right?
Edney: Yeah. And that’s a particularly rough one because many ingredients are imported, and then some of the drugs are then finished here, just like a car. All the pieces are brought in and then put together in one place. And so this is something the Trump administration has began the process of investigating. And PhRMA [Pharmaceutical Research and Manufacturers of America], the trade group for the drug industry, has come out officially, as you would expect, against the tariffs, saying that: This will reduce our ability to do R&D. It will raise the price of drugs that Americans pay, because we’re just going to pass this on to everyone. And so we’re still in this waiting zone of seeing when or exactly how much and all of that for the tariffs for pharma.
Rovner: And yet Americans are paying — already paying — more than they ever have. Maya, you have a story just about that. Tell us.
Goldman: Yeah, there was a really interesting report from an analytics data firm that showed the price that Americans are paying for prescriptions is continuing to climb. Also, the number of prescriptions that Americans are taking is continuing to climb. It certainly will be interesting to see if this administration can be any more successful. That report, I don’t think this made it into the article that I ended up writing, but it did show that the cost of insulin is down. And that’s something that has been a federal policy intervention. We haven’t seen a lot of the effects yet of the Medicare drug price negotiations, but I think there are signs that that could lower the prices that people are paying. So I think it’s interesting to just see the evolution of all of this. It’s very much in flux.
Rovner: A continuing effort. Well, we are now well into the second hundred days of Trump 2.0, and we’re still learning about the cuts to health and health-related programs the administration is making. Just in this week’s rundown are stories about hundreds more people being laid off at the National Cancer Institute, a stop-work order at the National Institute of Allergy and Infectious Diseases research lab at Fort Detrick, Maryland, that studies Ebola and other deadly infectious diseases, and the layoff of most of the remaining staff at the National Institute for Occupational Safety and Health.
A reminder that this is all separate from the discretionary-spending budget request that the administration sent up to lawmakers last week. That document calls for a 26% cut in non-mandatory funding at HHS, meaning just about everything other than Medicare and Medicaid. And it includes a proposed $18 billion cut to the NIH [National Institutes of Health] and elimination of the $4 billion Low Income Home Energy Assistance Program, which helps millions of low-income Americans pay their heating and air conditioning bills. Now, this is normally the part of the federal budget that’s deemed dead on arrival. The president sends up his budget request, and Congress says, Yeah, we’re not doing that. But this at least does give us an idea of what direction the administration wants to take at HHS, right? What’s the likelihood of Congress endorsing any of these really huge, deep cuts?
Raman: From both sides—
Rovner: Go ahead, Sandhya.
Raman: It’s not going to happen, and they need 60 votes in the Senate to pass the appropriations bills. I think that when we’re looking in the House in particular, there are a lot of things in what we know from this so-called skinny budget document that they could take up and put in their bill for Labor, HHS, and Education. But I think the Senate’s going to be a different story, just because the Senate Appropriations chair is Susan Collins and she, as soon as this came out, had some pretty sharp words about the big cuts to NIH. They’ve had one in a series of two hearings on biomedical research. Concerned about some of these kinds of things. So I cannot necessarily see that sharp of a cut coming to fruition for NIH, but they might need to make some concessions on some other things.
This is also just a not full document. It has some things and others. I didn’t see any to FDA in there at all. So that was a question mark, even though they had some more information in some of the documents that had leaked kind of earlier on a larger version of this budget request. So I think we’ll see more about how people are feeling next week when we start having Secretary Kennedy testify on some of these. But I would not expect most of this to make it into whatever appropriations law we get.
Goldman: I was just going to say that. You take it seriously but not literally, is what I’ve been hearing from people.
Edney: We don’t have a full picture of what has already been cut. So to go in and then endorse cutting some more, maybe a little bit too early for that, because even at this point they’re still bringing people back that they cut. They’re finding out, Oh, this is actually something that is really important and that we need, so to do even more doesn’t seem to make a lot of sense right now.
Rovner: Yeah, that state of disarray is purposeful, I would guess, and doing a really good job at sort of clouding things up.
Goldman: One note on the cuts. I talked to someone at HHS this week who said as they’re bringing back some of these specialized people, in order to maintain the legality of, what they see as the legality of, the RIF [reduction in force], they need to lay off additional people to keep that number consistent. So I think that is very much in flux still and interesting to watch.
Rovner: Yeah, and I think that’s part of what we were seeing this week is that the groups that got spared are now getting cut because they’ve had to bring back other people. And as I point out, I guess, every week, pretty much all of this is illegal. And as it goes to courts, judges say, You can’t do this. So everything is in flux and will continue.
All right, finally this week, Health and Human Services Secretary Robert F. Kennedy Jr., who as of now is scheduled to appear before the Senate Health, Education, Labor, and Pensions Committee next week to talk about the department’s proposed budget, is asking CDC [the Centers for Disease Control and Prevention] to develop new guidance for treating measles with drugs and vitamins. This comes a week after he ordered a change in vaccine policy you already mentioned, Anna, so that new vaccines would have to be tested against placebos rather than older versions of the vaccine. These are all exactly the kinds of things that Kennedy promised health committee chairman Bill Cassidy he wouldn’t do. And yet we’ve heard almost nothing from Cassidy about anything the secretary has said or done since he’s been in office. So what do we expect to happen when they come face-to-face with each other in front of the cameras next week, assuming that it happens?
Edney: I’m very curious. I don’t know. Do I expect a senator to take a stand? I don’t necessarily, but this—
Rovner: He hasn’t yet.
Edney: Yeah, he hasn’t yet. But this is maybe about face-saving too for him. So I don’t know.
Rovner: Face-saving for Kennedy or for Cassidy?
Edney: For Cassidy, given he said: I’m going to keep an eye on him. We’re going to talk all the time, and he is not going to do this thing without my input. I’m not sure how Cassidy will approach that. I think it’ll be a really interesting hearing that we’ll all be watching.
Rovner: Yes. And just little announcement, if it does happen, that we are going to do sort of a special Wednesday afternoon after the hearing with some of our KFF Health News colleagues. So we are looking forward to that hearing. All right, that is this week’s news. Now we will play my “Bill of the Month” interview with Lauren Sausser, and then we will come back and do our extra credits.
I am pleased to welcome back to the podcast KFF Health News’ Lauren Sausser, who co-reported and wrote the latest KFF Health News “Bill of the Month.” Lauren, welcome back.
Lauren Sausser: Thank you. Thanks for having me.
Rovner: So this month’s patient got preventive care, which the Affordable Care Act was supposed to incentivize by making it cost-free at the point of service — except it wasn’t. Tell us who the patient is and what kind of care they got.
Sausser: Carmen Aiken is from Chicago. Carmen uses they/them pronouns. And Carmen made an appointment in the summer of 2023 for an annual checkup. This is just like a wellness check that you are very familiar with. You get your vaccines updated. You get your weight checked. You talk to your doctor about your physical activity and your family history. You might get some blood work done. Standard stuff.
Rovner: And how big was the bill?
Sausser: The bill ended up being more than $1,400 when it should, in Carmen’s mind, have been free.
Rovner: Which is a lot.
Sausser: A lot.
Rovner: I assume that there was a complaint to the health plan and the health plan said, Nope, not covered. Why did they say that?
Sausser: It turns out that alongside with some blood work that was preventive, Carmen also had some blood work done to monitor an ongoing prescription. Because that blood test is not considered a standard preventive service, the entire appointment was categorized as diagnostic and not preventive. So all of these services that would’ve been free to them, available at no cost, all of a sudden Carmen became responsible for.
Rovner: So even if the care was diagnostic rather than strictly preventive — obviously debatable — that sounds like a lot of money for a vaccine and some blood test. Why was the bill so high?
Sausser: Part of the reason the bill was so high was because Carmen’s blood work was sent to a hospital for processing, and hospitals, as you know, can charge a lot more for the same services. So under Carmen’s health plan, they were responsible for, I believe it was, 50% of the cost of services performed in an outpatient hospital setting. And that’s what that blood work fell under. So the charges were high.
Rovner: So we’ve talked a lot on the podcast about this fight in Congress to create site-neutral payments. This is a case where that probably would’ve made a big difference.
Sausser: Yeah, it would. And there’s discussion, there’s bipartisan support for it. The idea is that you should not have to pay more for the same services that are delivered at different places. But right now there’s no legislation to protect patients like Carmen from incurring higher charges.
Rovner: So what eventually happened with this bill?
Sausser: Carmen ended up paying it. They put it on a credit card. This was of course after they tried appealing it to their insurance company. Their insurance company decided that they agreed with the provider that these services were diagnostic, not preventive. And so, yeah, Carmen was losing sleep over this and decided ultimately that they were just going to pay it.
Rovner: And at least it was a four-figure bill and not a five-figure bill.
Sausser: Right.
Rovner: What’s the takeaway here? I imagine it is not that you should skip needed preventive/diagnostic care. Some drugs, when you’re on them, they say that you should have blood work done periodically to make sure you’re not having side effects.
Sausser: Right. You should not skip preventive services. And that’s the whole intent behind this in the ACA. It catches stuff early so that it becomes more treatable. I think you have to be really, really careful and specific when you’re making appointments, and about your intention for the appointment, so that you don’t incur charges like this. I think that you can also be really careful about where you get your blood work conducted. A lot of times you’ll see these signs in the doctor’s office like: We use this lab. If this isn’t in-network with you, you need to let us know. Because the charges that you can face really vary depending on where those labs are processed. So you can be really careful about that, too.
Rovner: And adding to all of this, there’s the pending Supreme Court case that could change it, right?
Sausser: Right. The Supreme Court heard oral arguments. It was in April. I think it was on the 21st. And it is a case that originated out in Texas. There is a group of Christian businesses that are challenging the mandate in the ACA that requires health insurers to cover a lot of these preventive services. So obviously we don’t have a decision in the case yet, but we’ll see.
Rovner: We will, and we will cover it on the podcast. Lauren Sausser, thank you so much.
Sausser: Thank you.
Rovner: OK, we’re back. Now it’s time for our extra-credit segment. That’s where we each recognize the story we read this week we think you should read, too. Don’t worry if you miss it. We will put the links in our show notes on your phone or other mobile device. Maya, you were the first to choose this week, so why don’t you go first?
Goldman: My extra credit is from Stat. It’s called “Europe Unveils $565 Million Package To Retain Scientists, and Attract New Ones,” by Andrew Joseph. And I just think it’s a really interesting evidence point to the United States’ losses, other countries’ gain. The U.S. has long been the pinnacle of research science, and people flock to this country to do research. And I think we’re already seeing a reversal of that as cuts to NIH funding and other scientific enterprises is reduced.
Rovner: Yep. A lot of stories about this, too. Anna.
Edney: So mine is from a couple of my colleagues that they did earlier this week. “A Former TV Writer Found a Health-Care Loophole That Threatens To Blow Up Obamacare.” And I thought it was really interesting because it had brought me back to these cheap, bare-bones plans that people were allowed to start selling that don’t meet any of the Obamacare requirements. And so this guy who used to, in the ’80s and ’90s, wrote for sitcoms — “Coach” or “Night Court,” if anyone goes to watch those on reruns. But he did a series of random things after that and has sort of now landed on selling these junk plans, but doing it in a really weird way that signs people up for a job that they don’t know they’re being signed up for. And I think it’s just, it’s an interesting read because we knew when these things were coming online that this was shady and people weren’t going to get the coverage they needed. And this takes it to an extra level. They’re still around, and they’re still ripping people off.
Rovner: Or as I’d like to subhead this story: Creative people think of creative things.
Edney: “Creative” is a nice word.
Rovner: Sandhya.
Raman: So my pick is “In the Deep South, Health Care Fights Echo Civil Rights Battles,” and it’s from Anna Claire Vollers at the Louisiana Illuminator. And her story looks at some of the ties between civil rights and health. So 2025 is the 70th anniversary of the bus boycott, the 60th anniversary of Selma-to-Montgomery marches, the Voting Rights Act. And it’s also the 60th anniversary of Medicaid. And she goes into, Medicaid isn’t something you usually consider a civil rights win, but health as a human right was part of the civil rights movement. And I think it’s an interesting piece.
Rovner: It is an interesting piece, and we should point out Medicare was also a huge civil rights, important piece of law because it desegregated all the hospitals in the South. All right, my extra credit this week is a truly infuriating story from NPR by Andrea Hsu. It’s called “Fired, Rehired, and Fired Again: Some Federal Workers Find They’re Suddenly Uninsured.” And it’s a situation that if a private employer did it, Congress would be all over them and it would be making huge headlines. These are federal workers who are trying to do the right thing for themselves and their families but who are being jerked around in impossible ways and have no idea not just whether they have jobs but whether they have health insurance, and whether the medical care that they’re getting while this all gets sorted out will be covered. It’s one thing to shrink the federal workforce, but there is some basic human decency for people who haven’t done anything wrong, and a lot of now-former federal workers are not getting it at the moment.
OK, that is this week’s show. As always, if you enjoy the podcast, you can subscribe wherever you get your podcasts. We’d appreciate if you left us a review. That helps other people find us, too. Thanks as always to our editor, Emmarie Huetteman, and our producer, Francis Ying. Also, as always, you can email us your comments or questions, We’re at whatthehealth@kff.org, or you can still find me on X, @jrovner, or on Bluesky, @julierovner. Where are you folks hanging these days? Sandhya?
Raman: I’m on X, @SandhyaWrites, and also on Bluesky, @SandhyaWrites at Bluesky.
Rovner: Anna.
Edney: X and Bluesky, @annaedney.
Rovner: Maya.
Goldman: I am on X, @mayagoldman_. Same on Bluesky and also increasingly on LinkedIn.
Rovner: All right, we’ll be back in your feed next week. Until then, be healthy.
Credits
Francis Ying
Audio producer
Emmarie Huetteman
Editor
To hear all our podcasts, click here.
And subscribe to KFF Health News’ “What the Health?” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
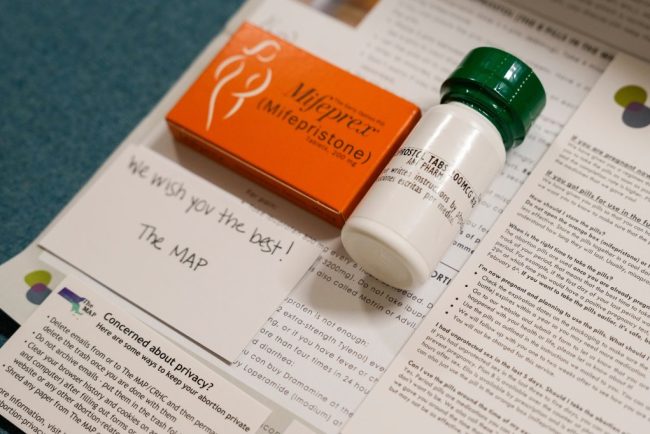
Despite Historic Indictment, Doctors Will Keep Mailing Abortion Pills Across State Lines
When the news broke on Jan. 31 that a New York physician had been indicted for shipping abortion medications to a woman in Louisiana, it stoked fear across the network of doctors and medical clinics who engage in similar work. “It’s scary. It’s frustrating,” said […]
Pharmaceuticals